Ischemic heart disease due to the effects of atheroma, causing narrowing or occlusion of one or more branches of the coronary arteries. Atheromatous plaques cause narrowing. Occlusion may be by plaque alone or plaques complicated by thrombosis. Narrowing of an artery leads to angina pectoris and occlusion to myocardial infarction.
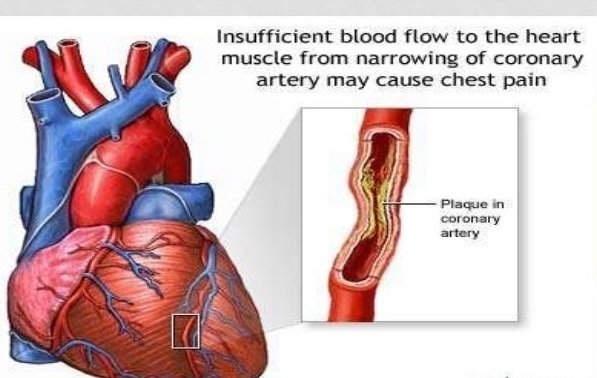
Angina pectoris
This is sometimes called angina of effort because the increase cardiac output required during extra physical effort causes severe chest pain, which may also radiate to the arms,neck and jaw. Insufficient blood flow to the heart muscle from narrowing of coronary artery may cause chest pain.
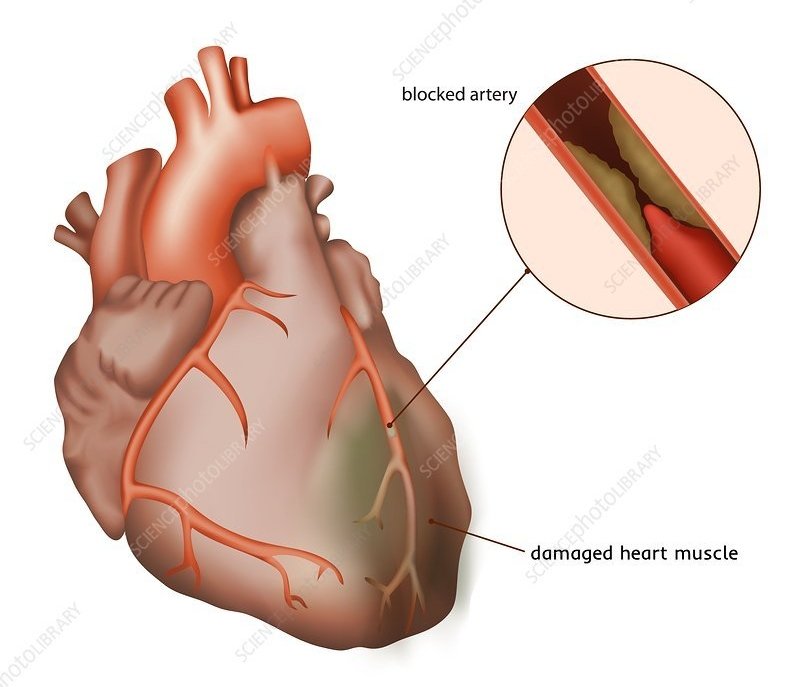
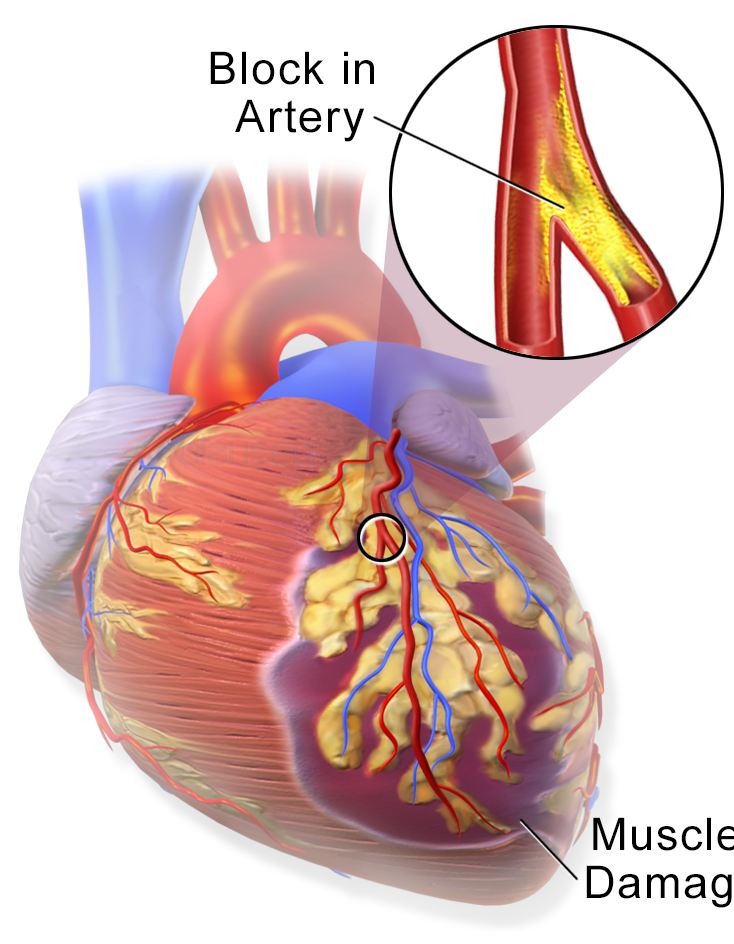
Myocardial infarction
The myocardium may infarct when a branch of a coronary artery is blocked.the commonest cause is an atheromatous plaque complicated by thrombosis. The extent of myocardial damage depends on the size of the blood vessels and site of the infarct.the damage is permanent because cardiac muscle cannot regenerate and the dead muscle is replaced with non functional fibrous tissue.
Symptoms of myocardial infarction
1. tightness in the chest
2. Chest pain which may also radiate to the arms,neck and jaw
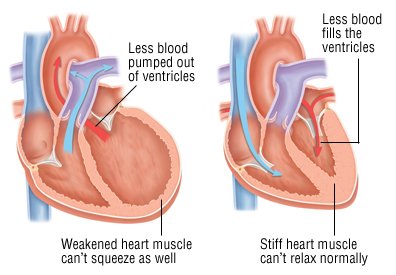
The heart is described as falling when the cardiac output is unable to maintain the circulation of sufficient blood to meet the needs of the body.
Compensatory mechanisms in heart failure
The heart failure happens actually, the body has little time to make compensatory changes,but if the heart fails over a period of time the following changes are likely to occur in an attempt to maintain cardiac output and tissue perfusion specially of vital organs.
1. The cardiac muscle fibers enlarge and increase in number, which makes the wall of the chambers thicker
2. The heart chambers enlarge
3. Deceased renal blood flow activates the resin angiotensin aldosterone system which leads to salt and water retention. This increase blood volume and cardiac workload. The direct vasoconstrictor action of angiotensin 2 increase peripheral resistance and puts further strain on the failing heart.
Acute heart failure
A sudden decrease in output blood from both ventricles causes acute reduction in the oxygen supply to the tissue. Recovery from the acute phase may be followed by chronic failure or death may occur due to anoxia of vital centres in the brain. Effects on body system are described below. The commonest causes are
1. Myocardial infarction
2. Pulmonary embolism
3. Severe cardiac arrhythmias
4. Rupture of heart chamber or valve cups
5. Severe malignant hypertension
Chronic heart failure
This develops gradually and in the early stages there may be not symptoms because compensatory changes. When compensation is not possible there is a gradual decline in myocardial efficiency. The commonest causes are:
1. Anaemia
2. Lungs disease
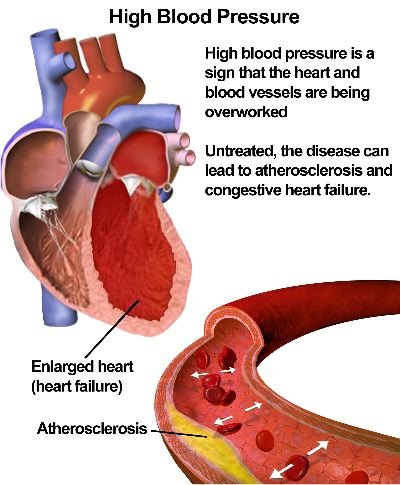
3. Hypertension or cardiac disease
Right side failure (congestive cardiac failure)
The right ventricle fails when pressure developed within it by the contracting myocardial is not enough to push blood through the lungs. When compensation has reached its limit and the ventricle can no longer empty completely the right atrium and venae cave becom congested with blood and this is followed by congestion throughout the venous system. The organs effected first are the liver, spleen and kidneys.this problems may be caused by increased vascular resistance in the lungs or weakness of the myocardium.
Resistance to blood flow through the lungs
It may be caused by
1. Pulmonary embolism
2. Left ventricular failure
3. Narrowing of the pulmonary valve
Weakness of the myocardium
This may be caused by ischaemia following infarction
Left ventricular failure
This occurs when the pressure developed in the left ventricle by the contracting myocardium is not enough to force blood into the aorta and the ventricle cannot then pump out all the blood it receives. causes include ischemic heart disease, which reduces the efficacy of the myocardium and hypertension.
The heart is a muscular organ . which pumps blood through the blood vessels of the the calculator system. The pumped blood carries oxygen and nutrients to the body, while carrying metabolic waste such as carbon dioxide to the lungs
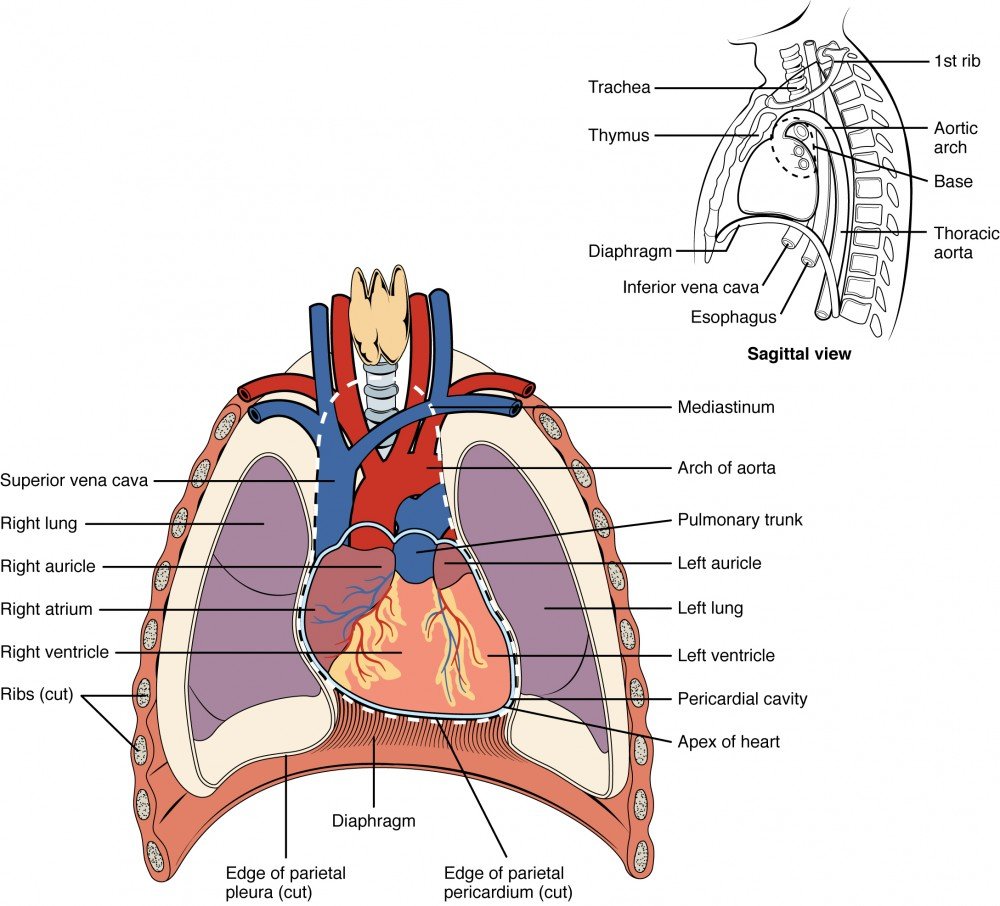
Location of the heart
The heart is located underneath the sternum in a thoracic compartment called the mediastinum, which occupies the space between the lungs.
size of the heart
Location of the heart
A human heart is roughly the size of a large fist. The heart weighs between about 10 to 12 ounces (280 to 340 grams) in men and 8 to 10 ounces (230 to 280 grams) in women.
Anatomy of the heart
anatomy of the heart & heart muscle
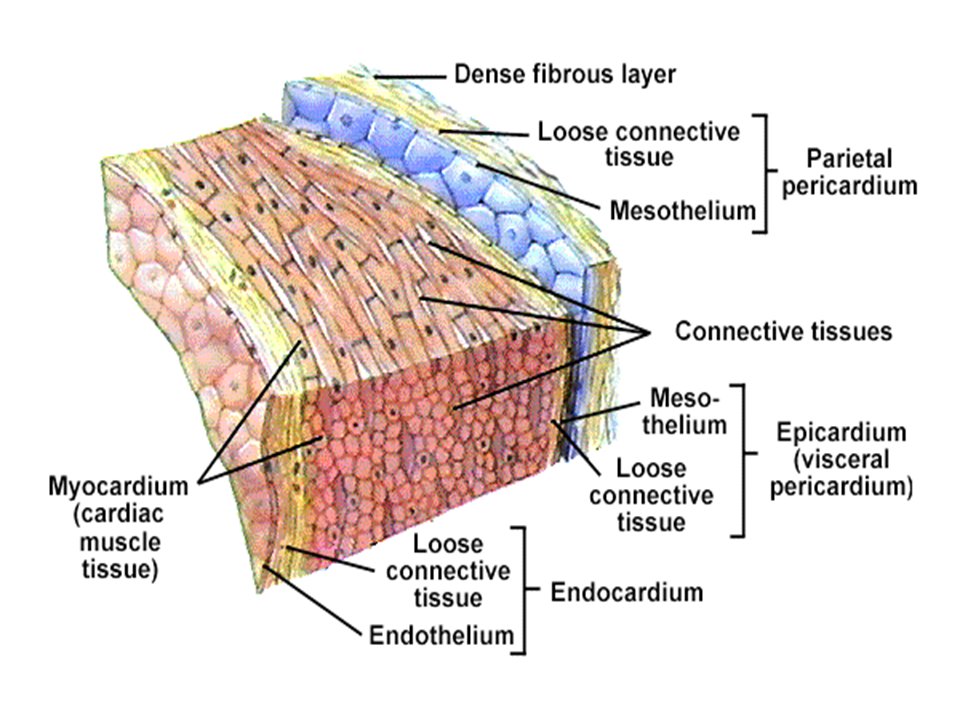
The heart wall is composed of three tissuelayers. Covering the outer surface of the heart is the epicardium. It is also referred to as the visceral pericardium, which is the inner layer of the pericardium . The epicardium is a serous membrane that consists of an external layer of simple squamous and an inner layer of areolar tissue (loose connective tissue). The squamous cellssecrete lubricating fluids in to the pericardial cavity.The thick middle layer of the heart wall is called the myocardium. It consists of numerous layers of cardiac muscle fibres that wrap around the heart wall. Contraction of the myocardium pumps blood out of the heart in to the aorta and pulmonary trunk arteries. Covering the outer surface of the heart wall is the endcardium. This layer also covers the heart valves and tendons and is continuous with the endothelium that lines the major blood vessels that attach to the heart.The endocardium is made up of thin layer of simple squamous cells and areolar tissue, similar to the epicardium. Secretions from the squamous cells help regulate the activity of the myocardium.
The Chambers of the Hearts
the chambers of the heart
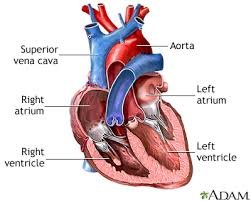
The heart is made up of four chambers. The superior chamber consists of the right atrium and the left atrium, which lie primarily on the posterior side of the heart.Extending anteriorly from each thin walled atrium is a small, ear-shaped appendage called auricle that expands the volume of the chamber. Blood drains into the atria from the pulmonary and systemic circulatory system. Composing the lower chambers are the right ventricle and left ventricle,which are much larger than the atria. The right ventricle pumps blood through the pulmonary circulatory system and the thicker walled left ventricle pumps blood through the longer systemic circulatory system. Internally, the two ventricles are separated by a thick myocardial wall called the interventricular septum On the anterior surface of the heart, the interventricular septum is marked by a shallow diagonal groove known as the anterior interventricular sulcus (or groove), which is occupied the anterior interventricular artery, great cardiac vein and adipose tissue.On the posterior surface of the heart, the ventricles are separated by the posterior interventricular sulcus, which contains the posterior interior artery, middle cardiac vein and adipose tissue.
The Circulation System
The Circulation System
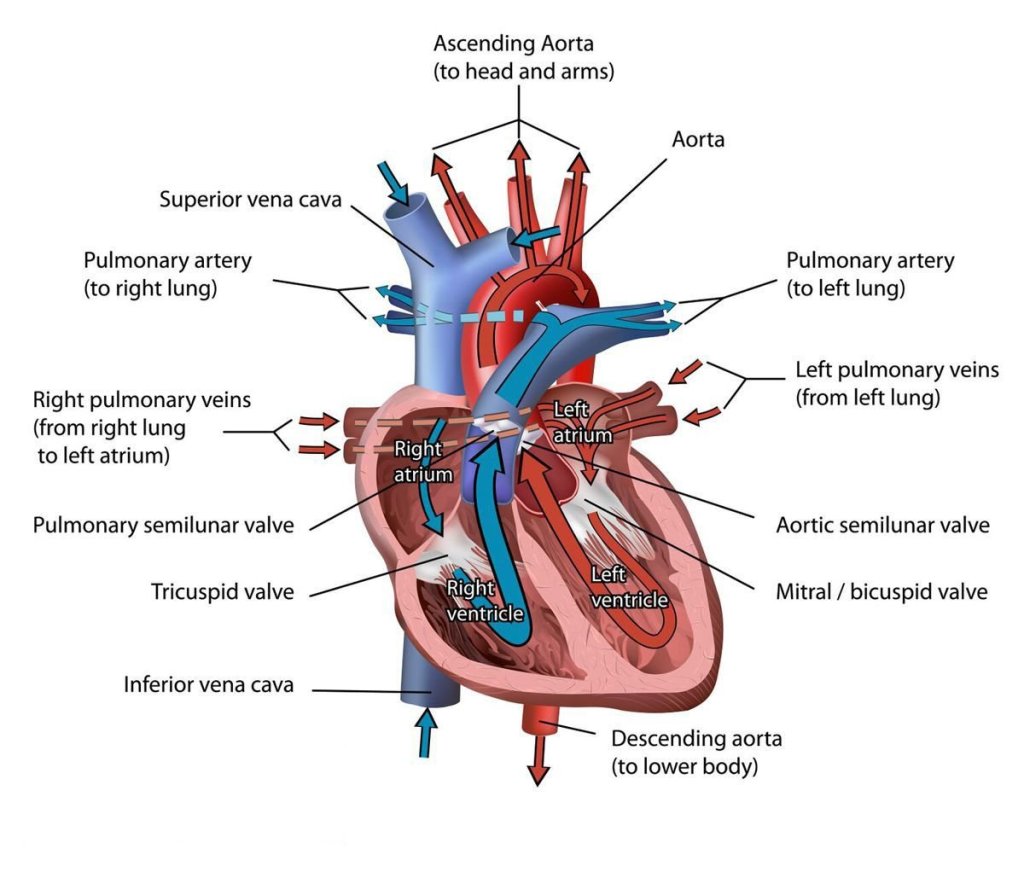
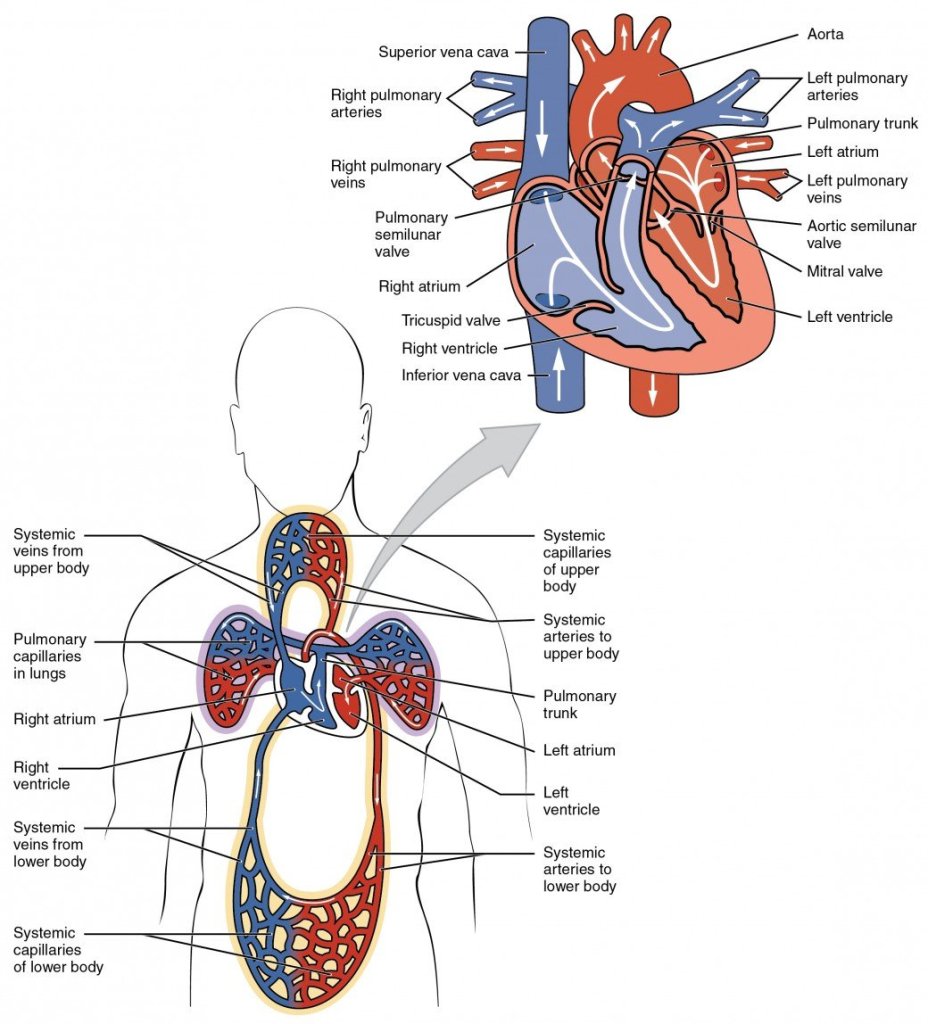
The major vessels of the heart are the large arteries and veins that attach to the atria, ventricles and transport blood to and from the systemic circulatory system and pulmonary circulation system. Blood is delivered to the right atrium from the systemic circulatory system by two veins. The superior vena cava transport oxygen-depleted blood from the upper extremities, heard and neck. The inferior vena cava transport oxygen-depleted blood from the thorax,abdomen and lower extremities. Blood exits the right ventricles through the pulmonary trunk artery. Approximately two inches superior to the base of the heart, this vessel branches into the left and right pulmonary arteries, which transport blood into the lungs. The left pulmonary veins and right pulmonary veins return oxygen-ated blood from the lungs to the left atrium.Blood passes from the left atrium into the left entricle and then is pumped into the systemic circulatory system through a large elastic artery called the aorta.
The Heart Valve Anatomy
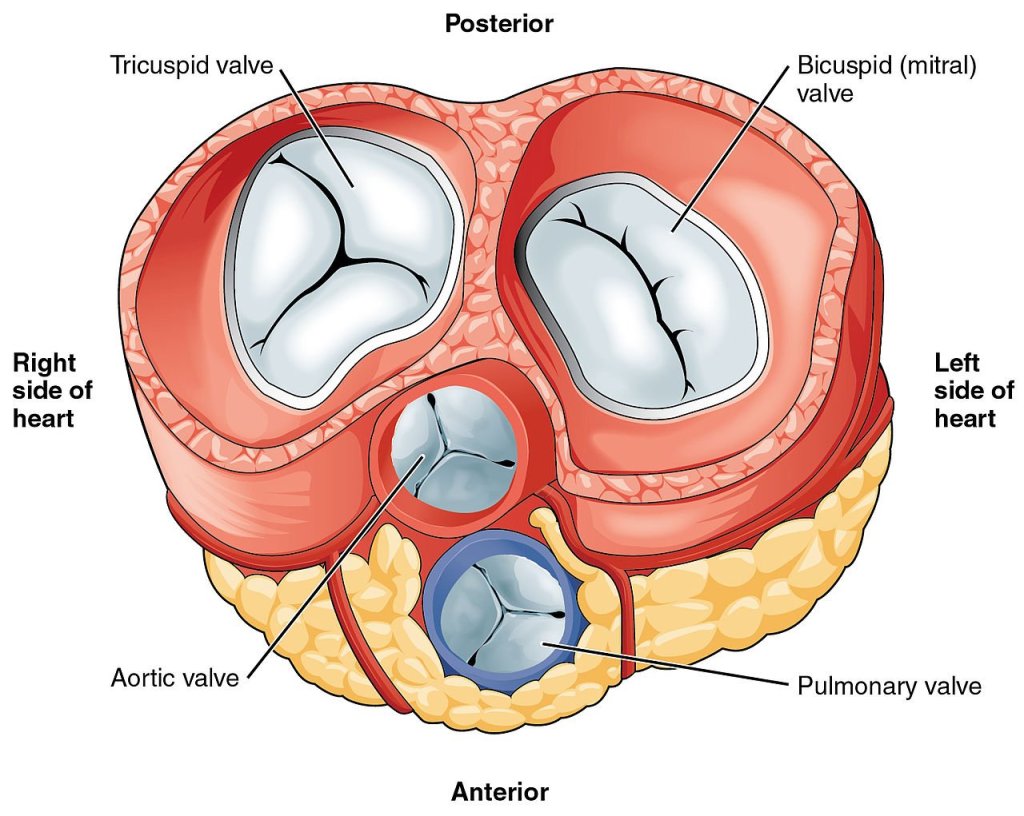
Four valves maintain the unidirectional flow of blood through the heart. The valves are located between each atrium and ventricle and in the two arteries that empty blood from the ventricle. These valves are primarily composed of fibrous connective tissues that originate and extend from the heart walls. The external surfaces of the valves are covered byendocardium. The Tricuspid valve (right atroventricular) is composed of three caps or flaps and controls blood flow from the right atrium to the right ventricle. The bicuspid valve is made up of two cusps or flaps and controls blood flow from the left atrium to the left ventricle. The term mitral valve is also commonly applied because the left AVvalve is shaped somewhat like a bishop’s miter. Thin tendon like cord called chordae tendineae connect the AV valves to cone shaped papillary muscles that extend upward from the myocardium. The chordea tendineae and papillary muscles tether the AV valves to the ventricular walls. This allows the valves to close properly and not bulge (or prolapse) into the atria. Semilunar valves direct blood flow from the ventricles into the aorta and pulmonary trunk artery. The valves are located in the vessels just above the opening to ventricles. Each consists of three cusps that curve upwards to from small pockets.The four heart valves open and close in response to pressure changes that occur in the ventricles during each cardiac cycle. When the ventricles relax their pressures drop below those of the atria, pulmonary trunk artery and aorta. This allows the AV valves to open as their cusps passively drop downwards. The pressure change additionally permits blood to flow into the ventricles from the atria without restriction. The semilunar valves close during this same period as blood flowing toward the ventricles collects in the pockets of the cusps. Closure of the semilunar valves prevents blood from re-entering the ventricles while they are relaxing. After filling with blood, the ventricles contract and their rising pressures forces blood up towards the atria and into the pulmonary trunk and aorta. Blood pushing up under the cusps causes the atrioventricular valves to close. As a result, blood enters the atria from the pulmonary veins but not from the ventricles. At the same time, rising pressure in pulmonary trunk artery and aorta forces the semilunar valves to open and blood flow into systemic and pulmonary circulatory systems. When the ventricles begin to relax, pressure in the chambers drop again and a new cardiac cycle begins
Coronary Arteries
The heart receives nutrients and gases from its own set of arteries, veins and capillaries called the coronary circulatory system. Blood enters the coronary circulatory system through the left coronary artery and the right coronary artery, which exit the aorta just above the cusps of the semilunar valves.After running a short distance between the pulmonary trunk artery and left auricle, the left coronary artery emerges onto the anterior surface of the heart. Near this point, it branches into the anterior interventricular artery (left anterior descending artery) and the left circumflex artery. The anterior interventricular artery lies in the anterior interventricular sulcus and gives off branches that supply blood to the anterior ventricles and anterior interventricular septum. The left circumflex artery runs along the coronary sulcus (between the left atrium and ventricle) to theposterior side of the heart, where it usually ends in an anastomosis with the right coronary artery. One or more left marginal arteries typically branch from the left circuflex artery as it travels around the heart. The left circumflex artery and its branches supply blood to the left atrium and the lateral and posterior portions of the left ventricles. The right coronary artery travels along the coronary sulcus (between the right atrium and ventricle) where it typically gives off smaller branches to the right atrium. AV nodes (80% of people) and SA nodes (5e5% of people). Larger right marginal arteries also diverge from the right coronary artery as it continues around the heart.The right marginal arteries supply blood to the lateral wall of the right ventricle. On the posterior surface of the heart, the right coronary artery typically (80%-85% of people) give rise to the posrterior interventricular artery (PIV) or posterior descending artery (PDA), which runs along the posterior interventricular sulcus and the posterior interventricular septum.
Coronary Veins
After flowing through the myocardium, most (80%) of the oxygen-depleted blood is returned to the right atrium by several prominent veins that run along the surface of the heart. Draining bloodfrom the anterior ventricle is the great cardiac vein. This vessel originates at the apex of the heart and runs superiorly along the anterior interventricular sulcus (next to the anterio interventricular artery). Near the right atrium, the great cardiac vein veers to the left and enters the coronary sulcus (between the left atrium and ventricle), where it extends to the back side of the heart. One or more left marginal veins typically merge with the great cardiac vein as it traverses the lateral ventricular wall. Small anterior cardiac veins also drain blood from the anterior right ventricle directly into the right atrium.Blood is removed from the lateral and posterior right ventricle (and atrium) by the small cardiac vein, which travels to the posterior surface of the heart in the coronary sulcus. Along its path, the small cardiac vein receives blood from the one or more right marginal veins.One the posterior side of the heart, the great and small cardiac veins merge with the coronary sinus, which empties into the right atrium. The coronary sinuses also receives blood from the middle cardiac vein that ascends along the posterior interventricular groove and the posterior vein of the left ventricle
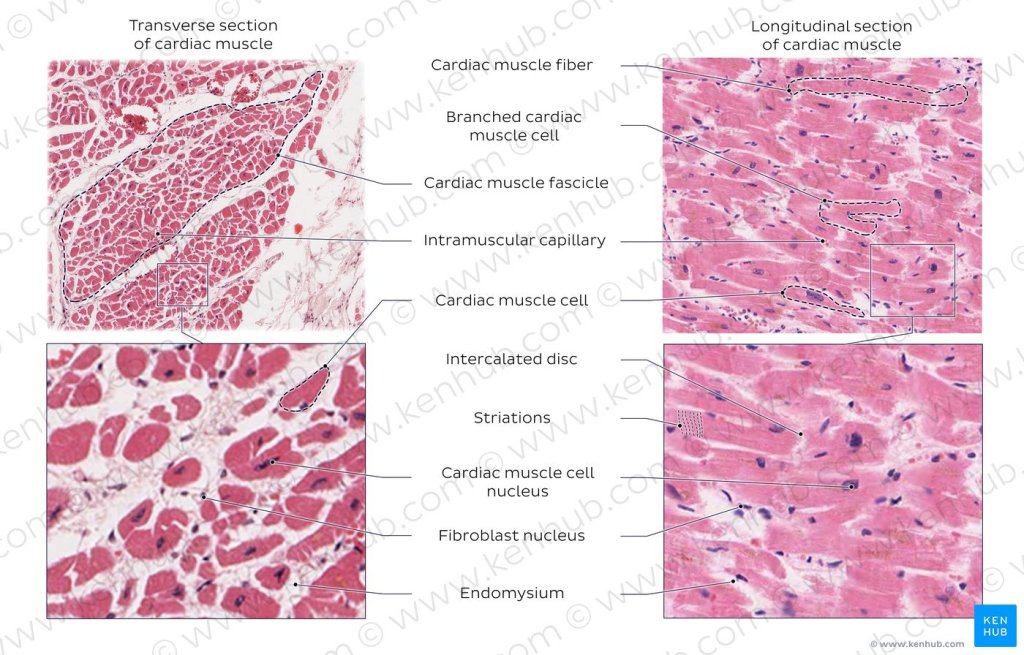
Cardiac Muscle Tissue
Cardiac muscle cells make up the myocardium portion of the heart wall. They are relatively short, branched fibers that measure approximately 10-20 micrometers in diameter and 50 to 100 micrometers in length. Typically each cardiac myocyte contains a single nucleus, which is centrally positioned.Thick and thin myofilaments are present and prganized into myofibrils. Their overlapping arrangement creates alternating dark (A) and light (I) bands or striations, similar to those seen in skeletal muscle tissue. Sarcoplasmic reticulum tubules surround the myofibrils. However, there are not well organised and do not have termial cisternae. T-tubules are also present, but run along the Z-discs (instead of the myofilament overlap zones). The mitichondria in cardiac myocytes are large and numerous. They supply the ATP needed for repeated contraction of the heart.Unlike other types of muscle tissues, cardiac myocytes are joined end to end by intercalated discs. These complex, highly convoluted couplings contain both anchoring junctions and electrical junctions. Forming the anchoring junctions are fascia adherens and desmosomes, which arrach the adjacent myocyte. The electrical junctions are composed of connexon protein channels, which usually occur in clusters referred to as gap junctions. Connexon proteins span the distance between adjacent plasma membranes and ions can travel through the channel pores. Th ion movement allows action potentials to pass directly from cell to cell. This property makes the entrie myocardium act like a single cell.
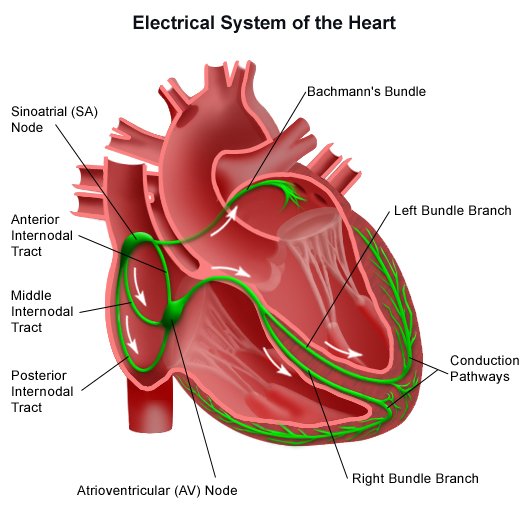
The Conduction System
The conducting system of the heart consists of cardiac muscle cells and conducting fibers (not nervous tissue) that are specialized for initiating impulses and conducting them rapidly through the heart. They initiate the normal cardiac cycle and coordinate the contractions of cardiac chambers. The conducting system provides the heart its automatic rhythmic beat. For the heart to pump efficiently and the systemic and pulmonary circulations to operate in synchrony, the events in the cardiac cycle must be coordinated. The sinoatrial (SA) node is a spindle-shaped structure composed of a fibrous tissue matrix with closely packed cells. It is 10-20 mm long, 2-3 mm wide, and thick, tending to narrow caudally toward the inferior vena cava. The SA node is located less than 1 mm from the epicardial surface, laterally in the right atrial sulcus terminalis at the junction of the anteromedial aspect of the superior vena cava (SVC) and the right atrium (RA).The middle internodal tract begins at the superior and posterior margins of the sinus node, travels behind the SVC to the crest of the interatrial septum, and descends in the interatrial septum to the superior margin of the AV node.The posterior internodal tract starts at the posterior margin of the sinus node and travels posteriorly around the SVC and along the crista terminalis to the eustachian ridge and then into the interatrial septum above the coronary sinus, where it joins the posterior portion of the AV node. These groups of internodal tissue are best referred to as internodal atrial myocardium, not tracts, as they do not appear to be histologically discrete specialized tracts.In 85-90% of human heart, the arterial supply to the AV node is a branch from the right coronary artery which originates at the posterior intersection of the AV and interventricular groove. In the remaining 10-15% of the heart, a branch of the left circumflex coronary artery provides the AV nodal artery. Fibres in the lower part of the AV node may exhibit automatic impulse formation. The main function of the AV node is modulation of the atrial impulse transmission to the ventricles to coordinate atrial and ventricle contractions
Bundle of His
The bundle of His is a structure that connects with the distal part if the compact AV node, perforates the central fibrous body and continues through the annulus fibrous, where it is called the non branching portion as it penetrates the membranous septum. Connective tissue of the central fibrous body and membranous septum encloses the penetrating portion of the AV bundle, which may send out extensions into the central fibrous body.Proximal cells of the penetrating portion are heterogeneous and resemble those of the compactAV node; distal cells are similar to cells in the proximal bundle branches. Branches from the anterior and posterior descending coronary arteries supply the upper muscular interventricular septum with blood, which makes the conduction system at this site more impervious to the ischemic damage, unless the ischemia is extensive.
Bundle branches
The bundle branches originate at the superior margin of the muscle interventricular septum, immediately below the membranous septum with the cells of the left bundle branch cascading downward as a continuous sheet onto the septum beneath the noncoronary aortic cusp. The right bundle branch continues intramycardially as an unbranched extension of the AV bundle down the right side of the interventricular septum to the apex of the right ventricle and base of the anterior papillary muscle. The anatomy of the left bundle branch system may be variable and may not conform to a constant bifascicluar division.
Punkinje fibers
Punkinje fibers connect with the ends of the bundle branches to form interwearving network on the endocardial surface of both ventricles. These fibers transmit the cardiac impulse almost simultaneously to the entrie right and left ventricle endocardium. Punkinje fibers tend to be less concentrated at the base of the ventricles and the papillary muscle tips and only penetrate the inner third of the endocardium. They appear to be more resistant to ischemia than ordinary myocardial fibers.
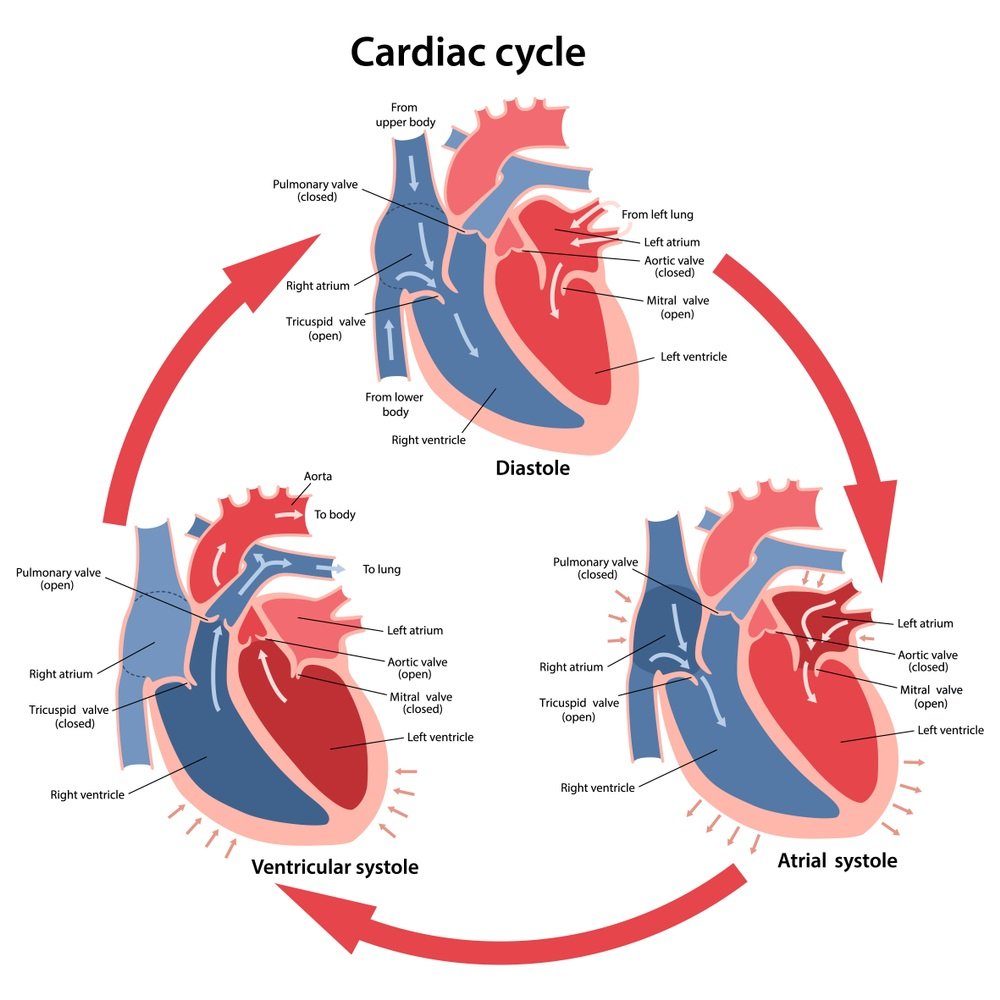
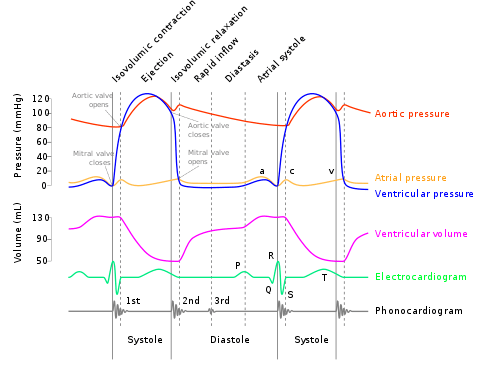
Cardiac Cycle
The cardiac cycle is the sequence of events that occur when the heart beats. The cycle has two main phases: diastole – when the heart ventricles are relaxed and systole – when the ventricles contract. In a cardiac cycle, blood enters the right atrium of the heart from the superior and inferior vena cavae, and flows across the tricuspid valve into the right ventricle. From the right ventricle the blood flows into the pulmonary artery, which is separated from the ventricle by the pulmonary valve. After oxygenation in the lungs, blood returns to the heart via four pulmonary veins that enter the left atrium. From the left atrium, blood flows across the mitral valve and into the left ventricle.From the left ventricle blood is ejected across the aortic valve into the aorta. Together, the mitral and tricuspid valves are known as the atrioventricular valves and the aortic and pulmonary valves as the semilunar valves .From a mechanical point of view, the cardiac cycle is due to blood movement as result of pressure differences within the chambers of the heart. In order for blood to flow through a blood vessel or through a heart valve, there must be force acting on the blood. This force is provided by the difference in blood pressure (a pressure gradient) across these structures by the contractions of the heart. Each heart beat, or cardiac cycle, is divided into two phases of contraction and relaxation, stimulated by elctricla impulses from the sinoatrial node (SA node). The time during which ventricular contraction occurs is called systole. The thime between ventricular contraction,wduring which ventricular filling occurs is called diastole 9also known as the relaxation phase). In early diastole, the ventricles relax, the semilunar valve close, the atrioventricular valves open and the ventricles fill with blood. In mid diastole, the atria and ventricles are relaxed, the semilunar valves are closed, the atrioventricular valves are open and the ventricles keep filling with blood. In late diastole, the SA node sends and electrical impulse to the atria, this causes the atria to contract and the ventricles to fill wit more blood. The electrical signal that causes contraction moves from the atria toward the ventricles. Before it does, it reaches the atrioventricular node (AV node). The AV node delays the signal so that the ventricles can contract all at once rather than a little bit at a time.Prior to systole, the electrical signal passes from the AV node down the AV bundl, also known as the bundle of His to the Punkinje fibers. The fibers allow the fast spread of the electrical signal to all parts of the ventricles and the electrical signal causes the ventricles to contract. Systole begins with the closure if the atrioventricular valves. During systole, the ventricles contract, the semi-lumar vwalves open and bloos is pumped from the ventricles to the aorta.Blood pressure is highest during systole and lowest during diastole. It has two components, the systole and diastole pressure. Normal systole pressure for an adult is estimates at 120 mmhg and normal diastole pressure is estimated at 80 mmhg
Cooking can sometimes feel like a chore at the end of a busy day. It’s often tempting to throw a ready meal in the oven or call for take out. But preparing a simple and healthy family meal doesn’t have to be hard or time-consuming. Here are some quick wholesome dishes that you and your family will love. They can even be prepared in advance.
I know, what could be better that a steaming plate of fries, gravy and cheese curd? Fries, gravy, cheese curd and bacon, that’s what! Throw in some fresh shallots, chilli, and a splash of roasted bone marrow and duck gravy, and we turn this popular French-Canadian dish into a something sublime.
During the week we’re often walking out the door with a coffee in one hand and slice of toast in the other, but on weekends breakfast is never rushed. It’s a late affair, sometimes spilling over to lunch, with lots of reading and chatter in between courses of fruits, poached eggs, honey and toast. One of our favorite things we like to serve when friends are visiting are buckwheat blueberry pancakes.
There’s nothing better than a warm bowl of pumpkin soup on a cold autumn day. Combine your roasted pumpkin with some onion, garlic, vegetable broth, and a few spices, and give it some time to simmer away. Pair it with a few slices of fresh bread to turn it into something sublime.